Knee Cartilage Damage and Restoration
A patient's guide to understanding what cartilage is, why it is difficult to treat, what the options are today, and how the right procedure is chosen.
This article is for educational purposes only. It is not a substitute for medical advice. Always consult your physician before starting or changing treatment.
What is a cartilage defect?
The knee joint is formed by three bones — the femur (thigh bone), tibia (shin bone), and patella (kneecap). The ends of these bones are covered by articular cartilage, a smooth, firm tissue that allows the bones to glide against each other with minimal friction.
A cartilage defect refers to a localized area of damage to this surface — think of it like a pothole in a road. The surrounding cartilage may be relatively healthy, but the damaged area disrupts the smooth joint surface and can cause significant symptoms. This is different from diffuse cartilage loss (osteoarthritis), which involves thinning across a larger area of the joint.
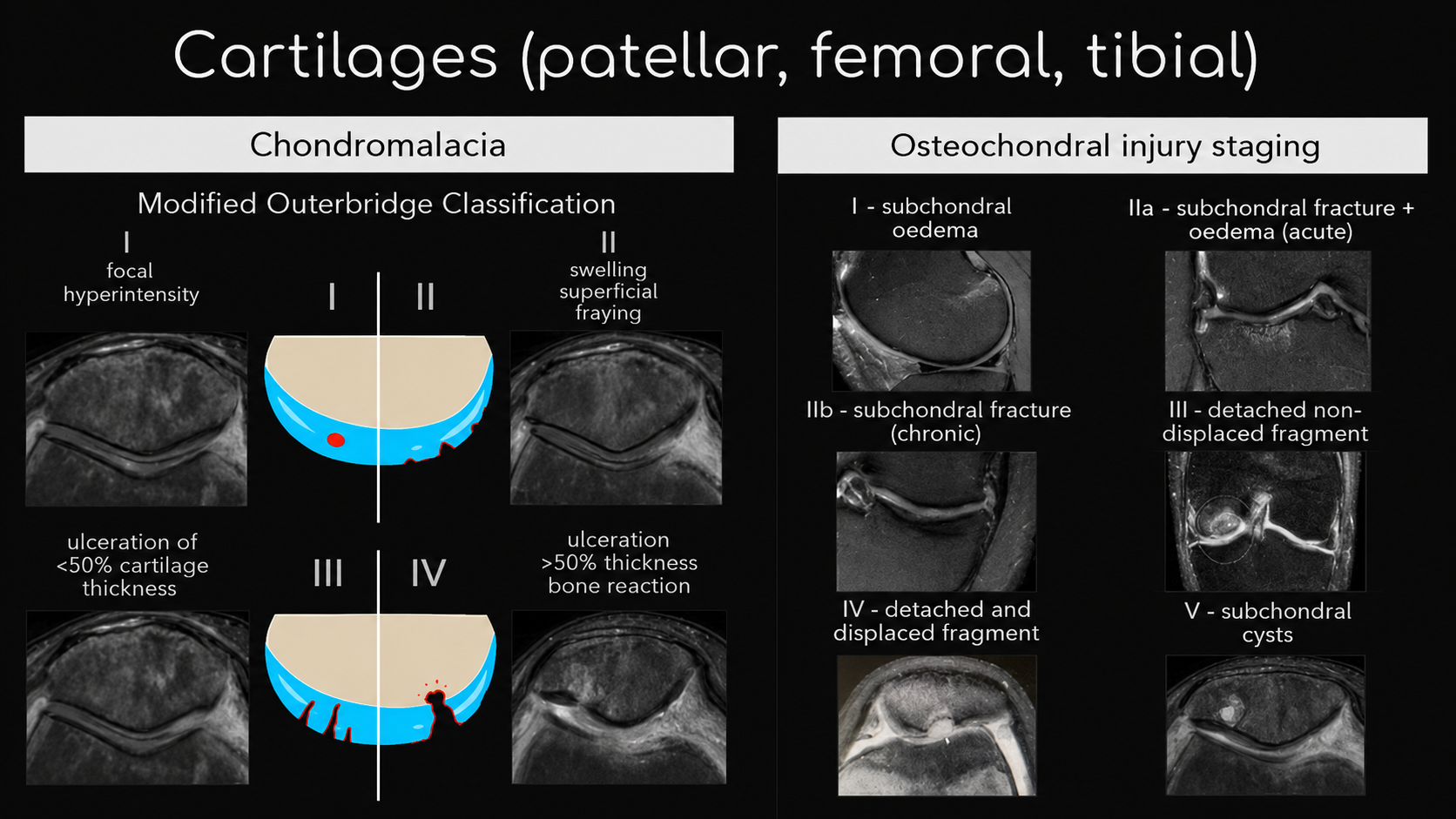
Focal cartilage defects are graded by severity on a scale of I to IV. Grade I represents surface-level softening or irregularity. Grade IV — the most severe — describes full-thickness cartilage loss down to the underlying bone. When the bone beneath the cartilage is also damaged, this is called an osteochondral injury.
Cartilage defects affect approximately 5–10% of people over the age of 40, but they also occur in younger patients following traumatic injuries.

What causes cartilage damage?
Focal cartilage damage is most commonly caused by an acute traumatic event — a sudden pivot or twist with a bent knee, a fall, or a direct blow to the joint. Sports that involve cutting, jumping, and contact carry a higher risk.
Cartilage can also be damaged gradually through repetitive stress or in the setting of other joint problems — malalignment, meniscus deficiency, or ligament instability — that alter how load is distributed across the joint surface.
Symptoms
Cartilage itself has no nerve supply and does not directly produce pain when damaged. Symptoms arise from the irritation of the bone beneath the cartilage and the joint lining (synovium) that results from cartilage loss. Symptoms can vary significantly depending on the size and location of the defect.
Common symptoms include:
• Joint pain — typically a dull ache with intermittent sharp pain, worsening with activity and improving with rest
• Stiffness — difficulty moving the knee through its full range of motion
• Crepitus — a grinding or grating sensation within the joint
• Catching or locking — may occur when a loose fragment of cartilage is present or the defect is large
• Swelling — particularly after activity
How is it diagnosed?
Diagnosis involves a combination of clinical examination and imaging.
A thorough physical examination assesses range of motion, areas of tenderness, joint line pain, swelling, and gait abnormalities. Weight-bearing X-rays evaluate joint space and the degree of any bony involvement. MRI provides detailed information about the size and depth of the defect, the status of the subchondral bone, and any associated injuries to the meniscus or ligaments.
The most accurate diagnostic tool is a diagnostic knee arthroscopy — a minimally invasive procedure in which a small camera is inserted into the joint. This allows direct visualization and precise measurement of the defect, and can be used to biopsy the area if further treatment planning is needed.
Why cartilage is uniquely difficult to heal
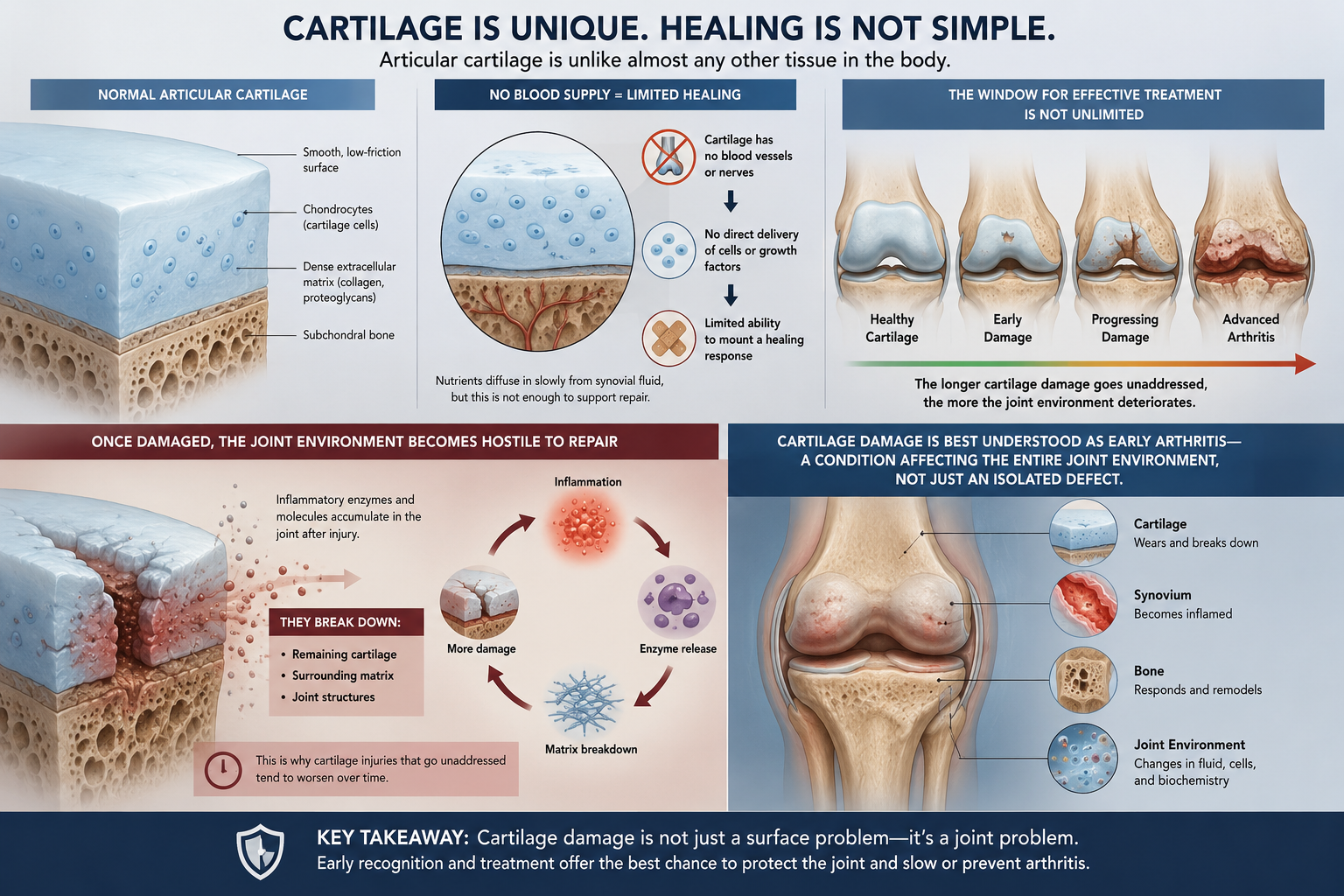
Articular cartilage is unlike almost any other tissue in the body. It has no blood supply. Without a blood supply, it cannot deliver the cells and growth factors needed to mount a healing response after injury.
Once cartilage is damaged, the joint environment can become actively hostile to repair. Inflammatory enzymes accumulate that break down both the remaining cartilage and the surrounding matrix. This is why cartilage injuries that go unaddressed tend to worsen over time — and why the window for effective treatment is not unlimited.
Cartilage damage is best understood as early arthritis — a condition affecting the entire joint environment, not just an isolated defect.
Non-surgical management
Not all cartilage defects require surgery. Some patients — particularly those with smaller lesions, lower activity demands, or significant other medical conditions — can be managed successfully without an operation.
Non-surgical options include:
• Activity modification — avoiding movements and activities that provoke pain
• Physical therapy — strengthening the muscles around the joint to offload the damaged area
• Anti-inflammatory medications — to reduce pain and swelling
• Corticosteroid injections — for short-term symptom relief
• Hyaluronic acid (gel) injections — to improve joint lubrication
• PRP (platelet-rich plasma) injections — an emerging option to support the joint environment
If non-surgical treatment resolves symptoms and allows return to desired activities, surgery is not needed.
When surgery is considered
Surgical intervention is typically considered when non-surgical treatment fails to relieve pain, when the patient is young and active with a significant defect, or when symptoms are functionally limiting and unlikely to improve without structural repair.
The goal of surgery is to restore the articular surface, reduce pain, and preserve the joint for as long as possible. It is not a cure for arthritis — but when the right procedure is matched to the right patient, it can meaningfully improve function and slow the progression of joint damage.
Surgical options
The surgical treatment of cartilage defects has evolved significantly over the past two decades. Today, several well-established procedures are available, each suited to a different patient profile and defect type.
The two-stage approach
Surgery for a cartilage defect often involves a two-stage approach. The first stage is a diagnostic arthroscopy — a minimally invasive procedure to directly visualize the defect, remove loose cartilage fragments, and smooth the damaged edges. Most patients experience meaningful symptom relief from this first stage alone.
If a definitive cartilage restoration procedure is indicated, it is typically performed no earlier than 6 to 8 weeks after the initial arthroscopy, once the joint has settled and the repair plan is finalized.
Understanding the two categories of cartilage surgery
All cartilage restoration procedures fall into one of two categories.
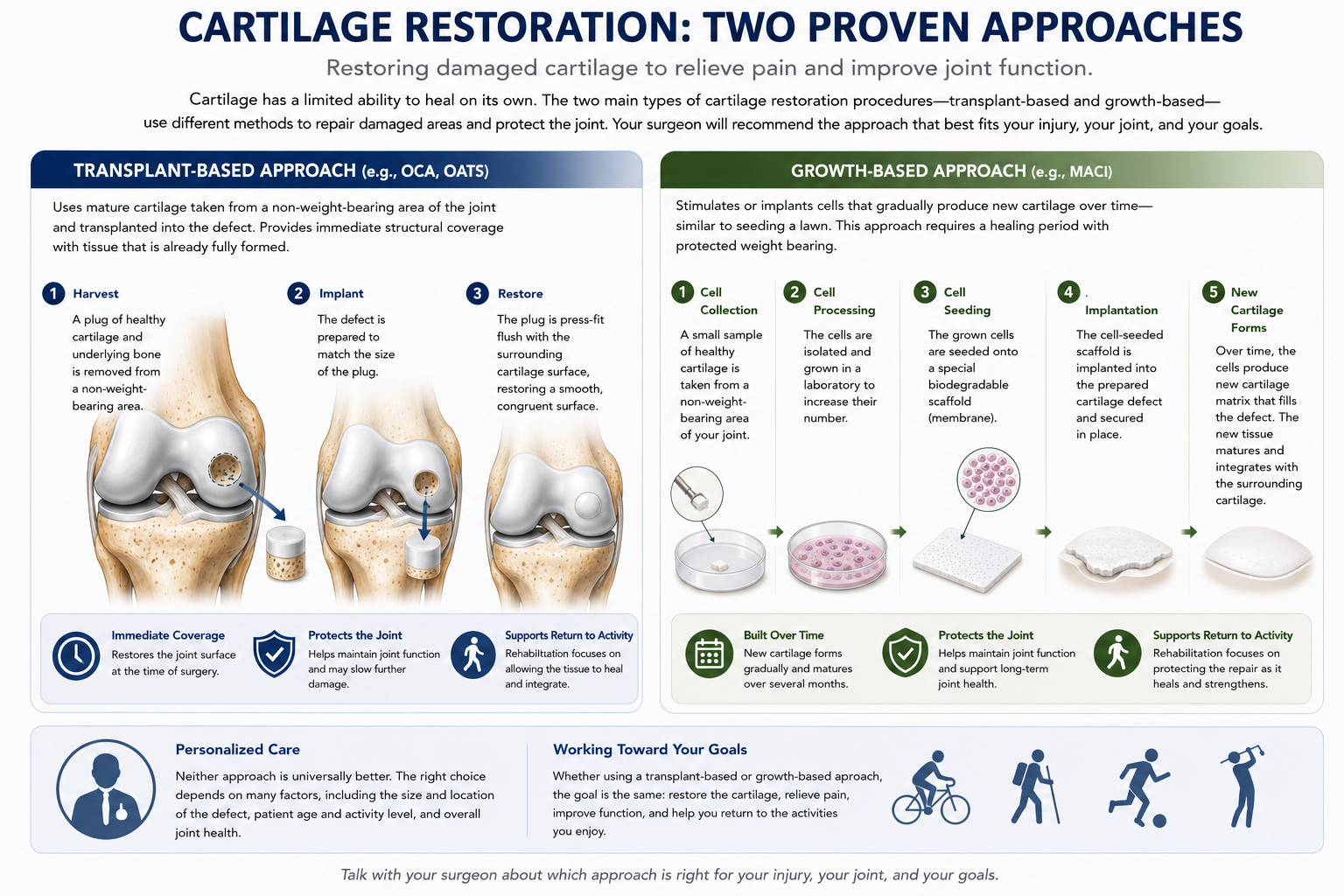
Growth-based procedures (such as MACI) stimulate or implant cells that gradually produce new cartilage tissue over time — like seeding a lawn. These procedures require protected weight bearing during the early healing phase.
Transplant-based procedures (such as OATS and OCA) place mature cartilage tissue directly into the defect — like laying sod. The result is immediate structural coverage using tissue that is already fully formed.
Neither approach is universally superior — the right choice depends on the individual patient, the defect, and the joint environment.
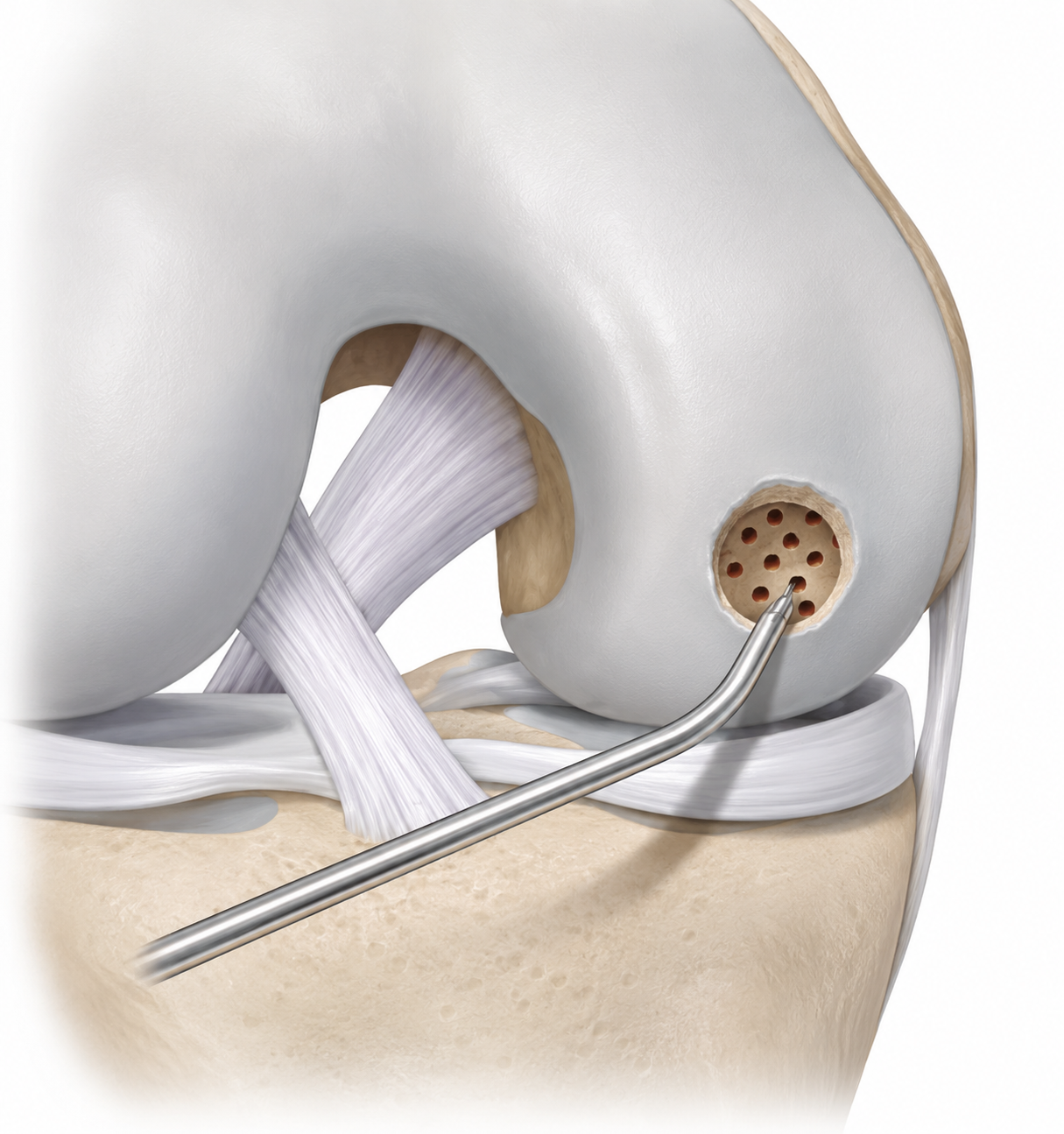
Microfracture — historical context
Microfracture involves creating small perforations in the subchondral bone to stimulate a healing response, producing fibrocartilage. Fibrocartilage is mechanically inferior to native hyaline cartilage and prone to breakdown in active patients. Its use has declined significantly over the past decade in favor of procedures that restore true cartilage tissue.
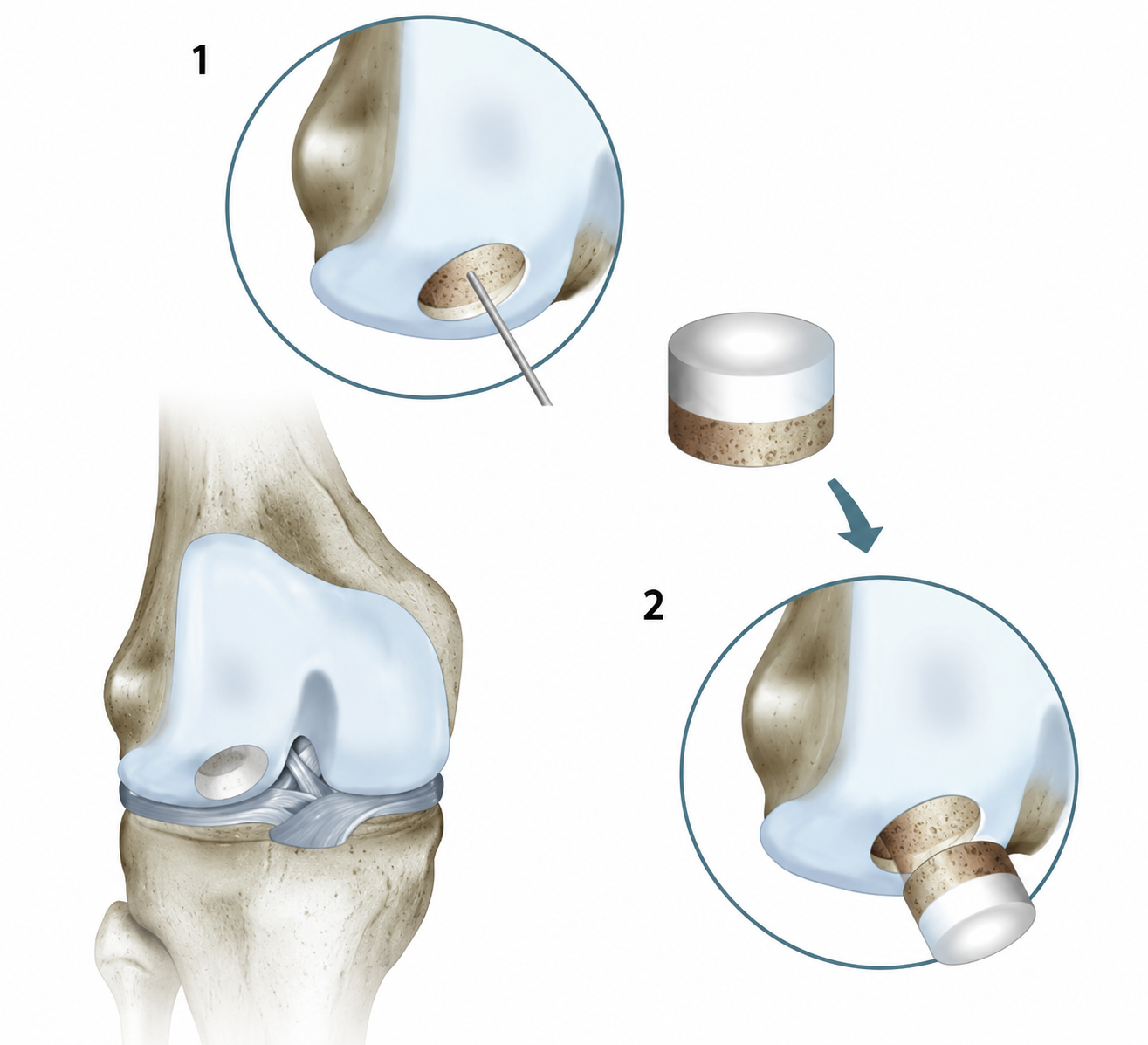
OATS — osteochondral autograft transfer
OATS involves harvesting a plug of healthy cartilage and bone from a low-demand area of the patient's own knee and transplanting it directly into the defect. Because the graft comes from the patient's own body, there is no risk of rejection. Best suited for smaller focal defects in active patients. Long-term follow-up data is favorable.
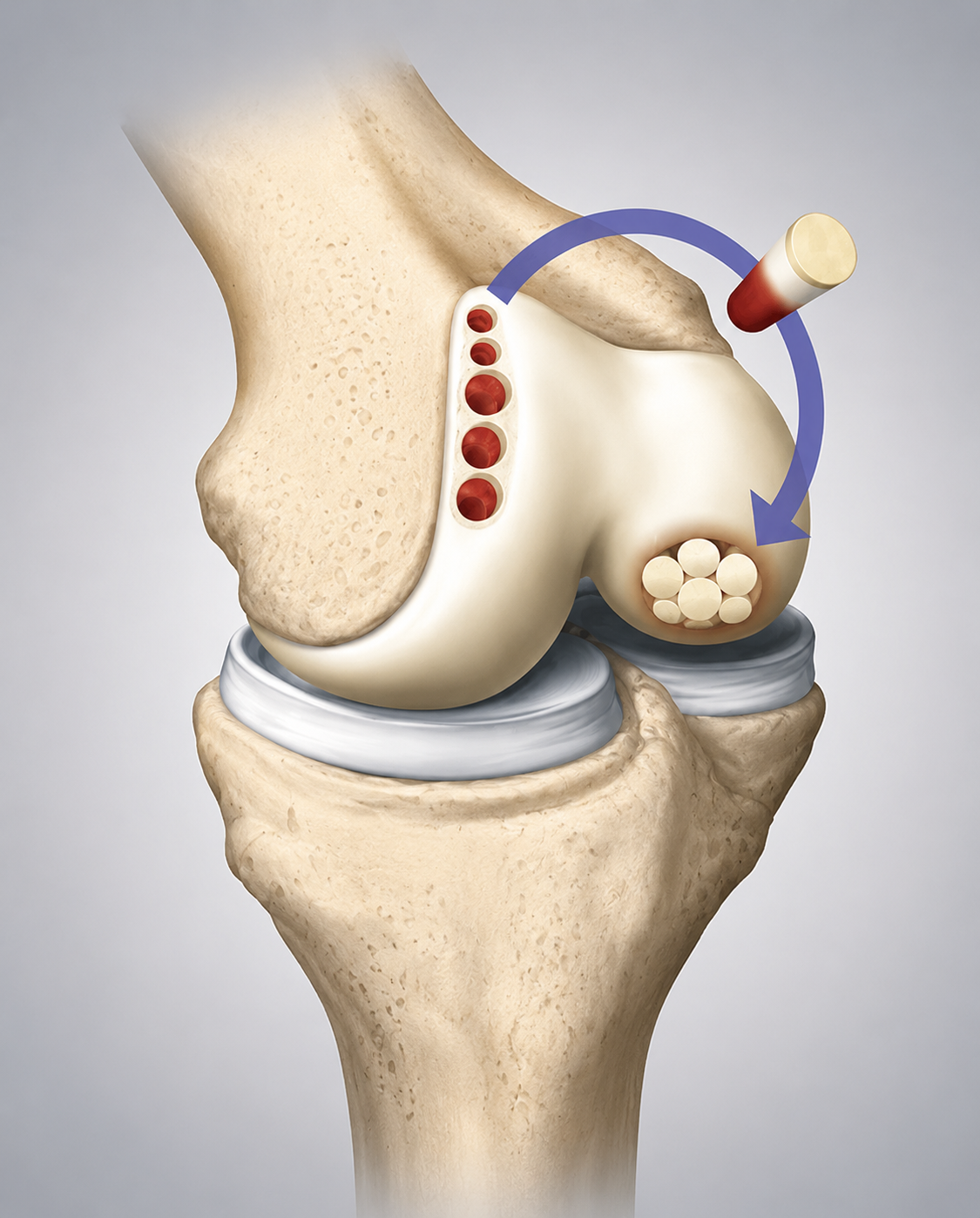
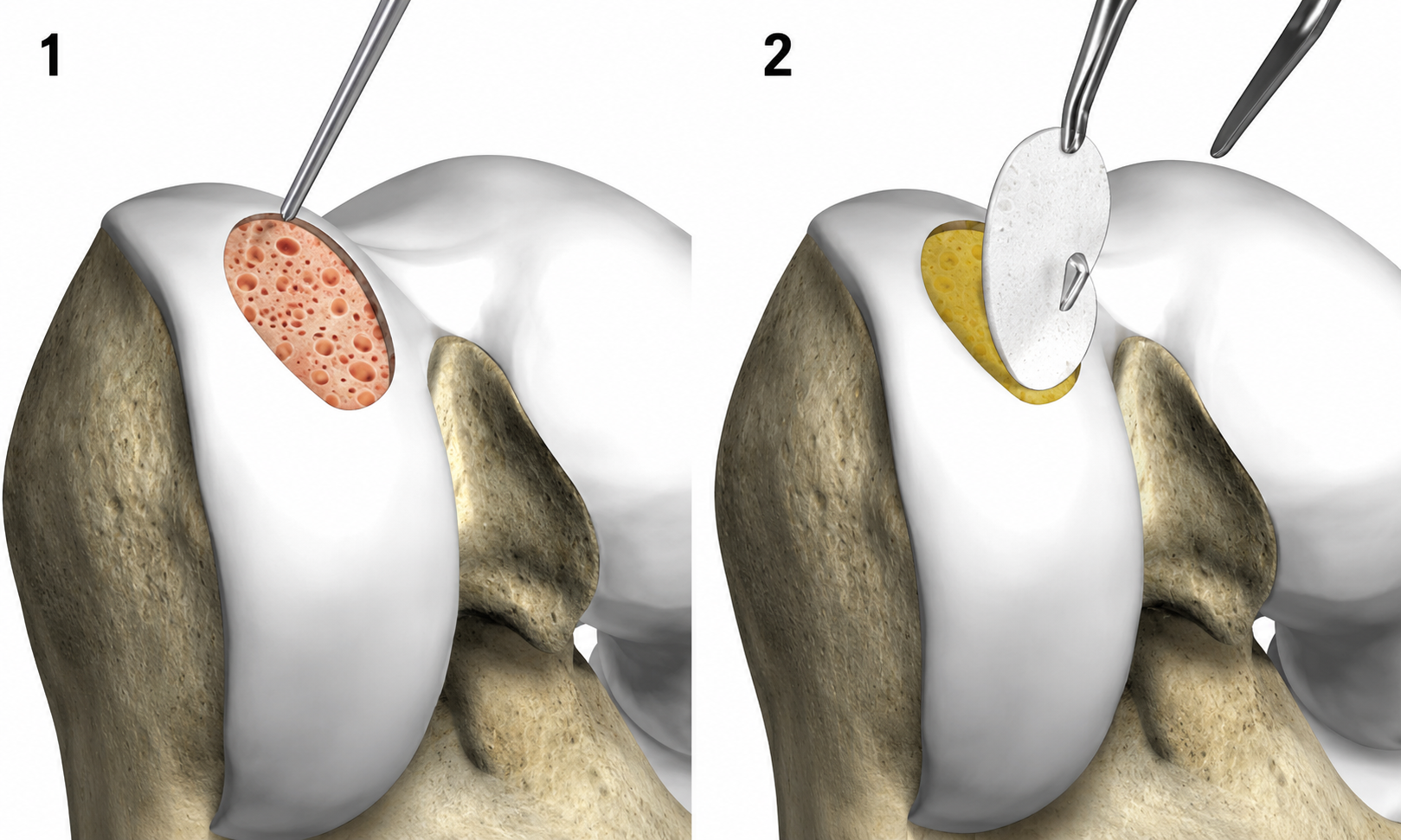
MACI — matrix-induced autologous chondrocyte implantation
MACI is a two-stage procedure. The patient's own cartilage cells are harvested, cultured in a laboratory on a collagen membrane, and then reimplanted into the defect. Most commonly used for superficial lesions and patellofemoral cartilage injuries. Suited for younger active patients who can commit to a structured rehabilitation program.
OCA — osteochondral allograft transplantation
OCA involves transplanting a full-thickness plug of mature cartilage and bone from a cadaveric donor directly into the defect — providing immediate coverage. Versatile across the femoral condyles, patella, and trochlea. Appropriate for a range of defect sizes. Survival rates reported to be excellent at 10-year follow-up.
CartiHeal (Agili-C) — scaffold-based regeneration
A next-generation biphasic scaffold supporting simultaneous regeneration of both cartilage and subchondral bone in a single procedure. No donor tissue required.

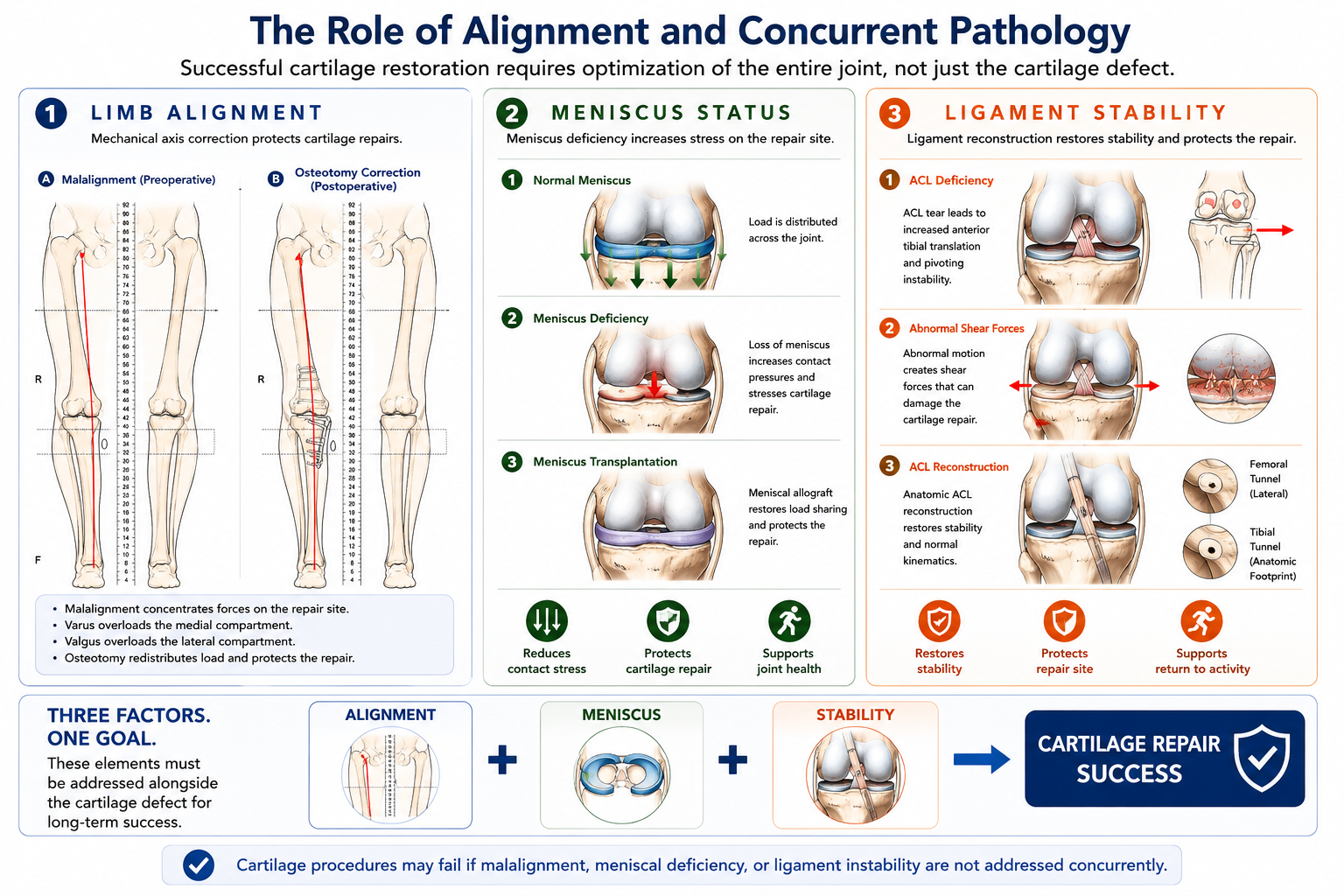
The role of alignment and concurrent pathology
Three factors must be evaluated alongside the cartilage defect itself:
• Limb alignment. Osteotomy may be performed concurrently to redistribute load and protect the repair long term.
• Meniscus status. Meniscus deficiency places excessive stress on the repair site. Meniscus transplantation may be indicated.
• Ligament stability. Ligament reconstruction should be addressed concurrently or prior to cartilage repair.
How the right procedure is chosen
The decision involves assessment of defect size and location, patient age and activity level, limb alignment, meniscus and ligament integrity, prior surgical history, and patient goals.
A thorough evaluation — including weight-bearing X-rays, MRI, and detailed clinical examination — is the foundation of a successful cartilage restoration plan.
Summary
Knee cartilage damage is a complex problem that requires individualized evaluation and treatment. The field has advanced significantly — from microfracture to OATS, MACI, OCA, and scaffold technology. For the right patient, modern cartilage restoration procedures can meaningfully reduce pain, restore function, and delay or prevent the need for joint replacement.
The most important step is an accurate diagnosis and a complete assessment of the joint environment — not just the cartilage defect itself.
James C. Messina, MD
Orthopedic Surgery · Sports Medicine · NYU Langone Long Island
Commack, NY · 631-919-6262
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Consult a qualified physician for evaluation and treatment of any medical condition.
References
Heir S, Nerhus TK, Røtterud JH, et al. Focal cartilage defects in the knee impair quality of life as much as severe osteoarthritis. Am J Sports Med. 2010;38:231-237.
Guermazi A, Hayashi D, Roemer F, et al. Partial- and full-thickness focal cartilage defects equally contribute to development of new cartilage damage in knee osteoarthritis: The Multicenter Osteoarthritis Study. Arthritis Rheumatol. 2017;69:560-564.
Slattery C, Kweon Y. Classifications in brief: Outerbridge classification of chondral lesions. Clin Orthop Relat Res. 2018;476:2101-2104.
Hsu RW, Himeno S, Coventry MB, Chao EY. Normal axial alignment of the lower extremity and load-bearing distribution at the knee. Clin Orthop Relat Res. 1990;255:215-227.
Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequence of a tear of the posterior root of the medial meniscus similar to total meniscectomy. J Bone Joint Surg Am. 2008;90:1922-1931.
Krych AJ, Hevesi M, Desai VS, Camp CL, Stuart MJ, Saris DBF. Learning from failure in cartilage repair surgery: An analysis of the mode of failure of primary procedures in consecutive cases at a tertiary referral center. Orthop J Sports Med. 2018;6:2325967118773041.
Anderson DE, Rose MB, Wille AJ, Wiedrick J, Crawford DC. Arthroscopic mechanical chondroplasty of the knee is beneficial for treatment of focal cartilage lesions in the absence of concurrent pathology. Orthop J Sports Med. 2017;5:2325967117707213.
Scillia AJ, Aune KT, Andrachuk JS, et al. Return to play after chondroplasty of the knee in National Football League athletes. Am J Sports Med. 2015;43:663-668.
Gudas R, Gudaite A, Mickevicius T, et al. Comparison of osteochondral autologous transplantation, microfracture, or debridement techniques in articular cartilage lesions associated with anterior cruciate ligament injury: A prospective study with a 3-year follow-up. Arthroscopy. 2013;29:89-97.
Bisson LJ, Kluczynski MA, Wind WM, et al. Patient outcomes after observation versus debridement of unstable chondral lesions during partial meniscectomy: The ChAMP randomized controlled trial. J Bone Joint Surg Am. 2017;99:1078-1085.
Churchill JL, Krych AJ, Lemos MJ, Redd M, Bonner KF. A case series of successful repair of articular cartilage fragments in the knee. Am J Sports Med. 2019;47:2589-2595.
Wu IT, Custers RJH, Desai VS, et al. Internal fixation of unstable osteochondritis dissecans: Do open growth plates improve healing rate? Am J Sports Med. 2018;46:2394-2401.
Barrie HJ. Hypertrophy and laminar calcification of cartilage in loose bodies as probable evidence of an ossification abnormality. J Pathol. 1980;132:161-168.
Bauer KL. Osteochondral injuries of the knee in pediatric patients. J Knee Surg. 2018;31:382-391.
Steadman JR, Rodkey WG, Briggs KK. Microfracture: Its history and experience of the developing surgeon. Cartilage. 2010;1:78-86.
Steadman JR, Rodkey WG, Rodrigo JJ. Microfracture: Surgical treatment and rehabilitation to treat chondral defects. Clin Orthop Relat Res. 2001;391(Suppl).
Krych AJ, Saris DBF, Stuart MJ, Hacken B. Cartilage injury in the knee: Assessment and treatment options. J Am Acad Orthop Surg. 2020;28(22):914-922. doi:10.5435/JAAOS-D-20-00266.